

So, you're curious about Ozempic.

This post originally appeared on Health Shift, Dr. Alice Burron’s Substack.
Good morning, health heroes!
Welcome to this morning’s edition of Health Shift. Things have been crazy out in the world of health — doesn’t it always seem like once you’ve got a handle on the latest fad, something else comes along to confuse you?
You may have been hearing about GLP-1’s, like Wegovy (called Ozempic when used for Type 2 Diabetes), Saxenda, and Zepbound. It has been in the news frequently lately, surrounding the many, many celebrities who have used it for weight loss.
In fact, a recent study shows that 1 in 8 people have used Ozempic, and if you don’t take it yourself, you likely know someone who does.
It’s my job and passion in life to help people harness self-awareness and self-mastery to make better health decisions. Our decisions shape our future and smart health decisions lead to promising health opportunities, faster healing, and improved lives.
This open-ended question about Ozempic seemed like a perfect opportunity to try and navigate using The Health Navigator approach. Clients and friends all seemed to have questions surrounding this fad: should I try it, is it safe, is it too good to be true?
Well, I thought. Let’s find out.
The Parameters
I gave myself 48 hours to do a deep-dive into Ozempic and other GLP-1 weight loss drugs, and I had to use my own set of analytical and critical thinking skills — the same that I teach and coach with here at The Health Navigator Group — to do so.
I wanted to come up with a well-rounded answer for myself (would I ever consider taking a GLP-1?) and for my clients (would I recommend that they take it?).

I’m going to be real and transparent with you.
Doing this exercise (and writing about it in a very public forum) took a considerable amount of vulnerability, putting my own biases rather uncomfortably on display. When I encourage my clients to do this, it’s within the privacy of their own work or with their health coach.
For the sake of this experiment, I’m going to go ahead and put mine on here on paper — thank you in advance for your respect. I want to cultivate a healthy space to work through health biases and challenges so that anyone — and I do mean anyone — can solve their health problems through self-awareness and self-advocacy.
Why 48 hours? I wanted to do this exercise in the typical period of time that it would take a person with a moderate health issue (not severe) who is motivated to make a decision do so. It’s a more generous amount of time than a quick Reddit forum search, but not so long it takes weeks to come to a decision.
This means I’m really trying to emulate someone who is genuinely considering this medication in a realistic time frame. I won’t go to the university library and find all of the research articles like I would a research paper, although that is tempting.
Let’s see if I can reach a worthwhile conclusion given those parameters.
(If you’re short on time and want to skip to the conclusion, just scroll to the end. There’s a lot of great info in the middle, return whenever you’d like!)
Let’s face it. I’m definitely biased when it comes to Ozempic.
First of all, the fact is, I’m in the business of preventing disease and keeping people healthy.
As a physiologist, personal trainer, and from a health coach perspective, I am all about leveraging the core aspects of health, such as incorporating exercise, smart eating, stress management, maintaining adequate sleep quality and quantity, and time management as the first-line defense against disease.
I have researched the evidence and I know that managing these variables almost always results in weight loss, but it takes time and perseverance. I have also helped my clients lose collectively hundreds of pounds. So, I come to the table with this perspective, and it may become barrier to my objectivity.
Bias 1: The Illusion of Control
The first bias I can name immediately. It’s the illusion of control, where I think people have control over their lifestyle behaviors and aren’t victims to their desires (i.e. they aren’t helpless to overcoming the urge to consume large amounts of unhealthy food, and they can become more active).
There might be instances where weight loss using the standard approach is nearly impossible, such as when dealing with a psychological or physical disorder, but I tend to think that the majority of people are able and equipped to lose weight without medications. They may need to think creatively if they don’t have resources like a gym or healthy food nearby, but there are always options. That’s what I generally think.
Bias 2: Representative Bias
I also have representative bias where I can’t appropriately assess the likelihood of my anticipated concerns with this medication will actually happen because I’m using only what I know to compare this scenario to and it’s largely based on my experience.
However, I do have a lot of experience working with people and weight loss, and I am a student of the health trends.
I also am coming with one large, insurmountable bias – I’m not overweight. But I’ve been overweight before to the tune of 35 pounds (and I honestly could lose about 5 – 8 pounds now). In the past, I’ve lost my weight through lifestyle management, so I know it can be done.
I’m sure there are more biases, but I’ll try to stay aware as I move forward in my analysis of GLP-1s.
(You can find the list of health biases that I use to check myself here on our free resources page.)
My emotional ties to the subject of GLP-1’s.
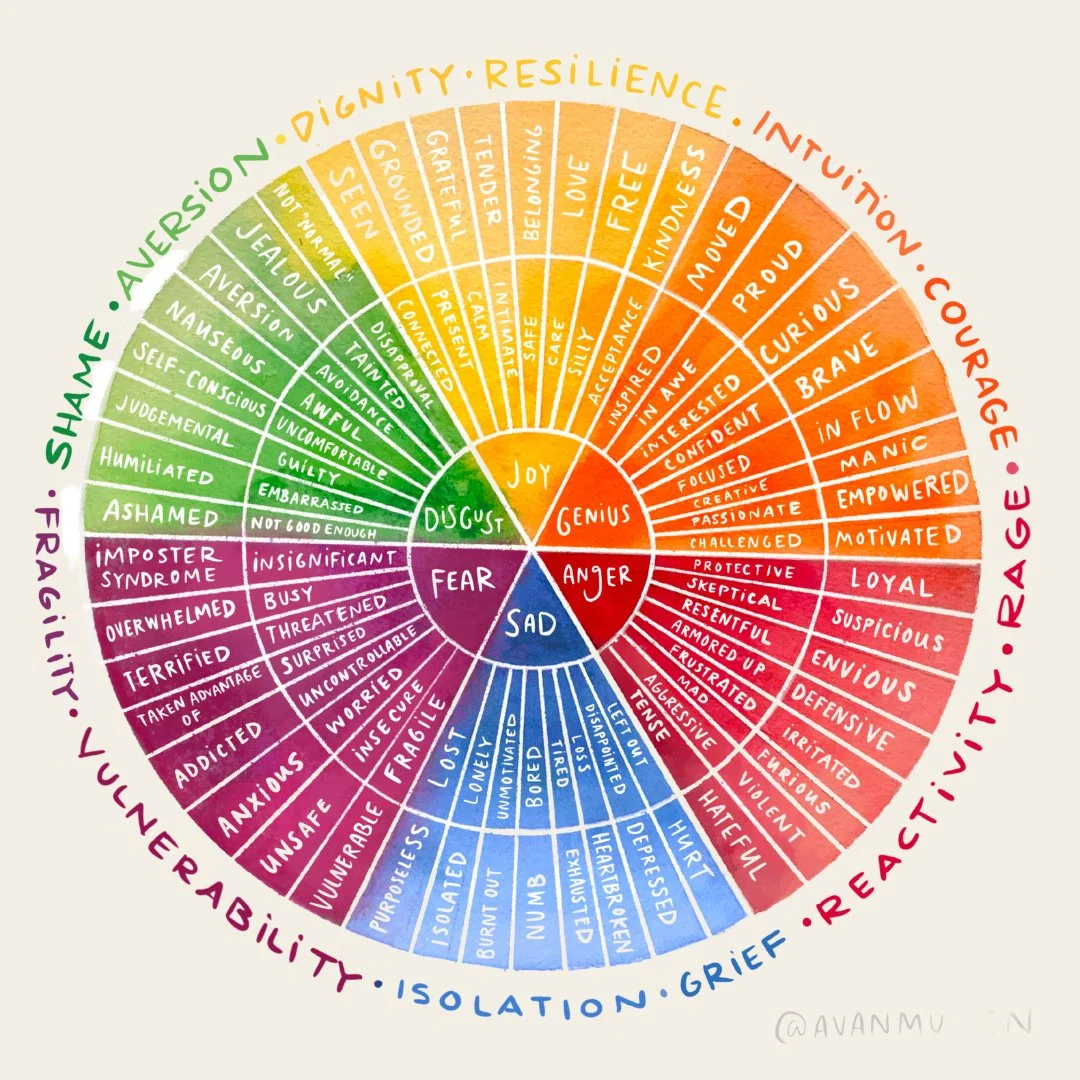
The Emotions Wheel
I have emotions tied to this topic.
Inherently, I came in with an underlying feeling of frustration… and even, surprisingly, anger. I went to the emotion wheel and found more specific words that I associated with my response. This is something I encourage all of my clients to tap into using the Emotion Wheel (above) to help.
I’m feeling skepticism, defensiveness, irritation, suspiciousness, fear, and a little disgust.
However, I also feel challenged, moved, empowered, motivated, confident, inspired, and interested in this topic.
I recognize that I really care about people, and I want them to think through this topic with objectivity. Obviously, I can’t be 100% objective myself, so I’m going to have to do my best, but it’s a real barrier to our thinking and this is always going to be a challenge when we make health decisions.
I’m going to touch on where these feelings are coming from, so you get some understanding of the barriers I’m dealing with as I try to navigate my opinion on these medications.
Where are these feelings coming from?
Alright, let’s work backwards and figure out why these emotions popped up. First, I feel as if lifestyle modifications continually get swiped aside and poor health behaviors are put in the light of acceptable and tolerable.
Lifestyle behaviors are not addressed as a first-line approach when we discuss medications – they become second.
Yes, the recommendation is to take GLP-1s in tandem with lifestyle approaches, but I’m finding that few are doing so (based on GLP-1 forums where many tout weight loss without doing anything). We are not adequately addressing the cause of the obesity and diabetes epidemic.
On a personal level, I believe that, as a society, if we keep focusing on a quick fix approach to being healthy, our health as a nation will continue to decline.
We must focus on cultural and societal prevention interventions alongside individual treatments. These medications are an option, but they’re not the magic cure – there is no fix that works in isolation without repercussions (both good and bad), and from GLP-1s we have yet to discover how other physiological systems will respond to this new approach to weight management.
From the research, it looks like many physiological systems are benefiting from the weight loss provided by GLP-1s – a decrease in the risk of heart disease and diabetes are a few examples, not to mention the psychological benefit of looking better. That is why researchers, and the medical community are excited about them.
This showcases the benefits of weight loss on health and underlines the need for us to lose weight as an overall nation. But I can’t help but ask, how can we find ways that are not just medical, but don’t cost money? (Especially considering Ozempic’s whopping $1k per month!) Weight loss is an important tool for our overall health, and I believe we can all access it through lifestyle.

A very literal example of a kinetic chain.
As a physiologist, I also think in terms of kinetic chains.
Kinetic chains are how the muscles and joints work together to move our bodies. If you hurt one part of your body, like a knee, then you’ll walk differently and the hip on your other side will hurt, then your back, etc.
Overlay this concept to other physiological systems. If you take a medication that impacts the endocrine system (the chemical messengers of the body) like GLP-1s do, then what else gets impacted? The answer is: every other system because they’re all linked, and some will begin to limp because now the body is functioning differently.
I think we should be talking about this aspect of the medication and its unintentional negative consequences.
My initial questions and concerns around GLP-1’s.
I took the time to thoroughly consider my concerns around these weight loss drugs, including the social repercussions of their side effects. My list of concerns looked like this:
🫕 People who don’t want to eat or drink might be less likely to socialize. That concerns me since we have what many are calling a loneliness epidemic. Food brings people together and creates endorphins which counters negative emotions. How much will socialization will be impacted?
👩🏽🍳 This also impacts the restaurant industry. People losing the desire to eat (and socialize around food) changes our relationship to restaurants.
💰The cost of GLP-1s is about $1000 a month. Will people go broke because they’re taking this medication? Will they be able to afford to stay on it as long as they are suggested to do so? What about those who can’t afford it?
💵 How will health insurance handle this? How will corporate employers who sponsor health insurance deal with it? Will it make health insurance even more unaffordable?
💉 There is a shortage of GLP-1s because pharmaceutical companies are struggling to keep up with demand. Doctors are starting to prioritize diabetics first, then weight loss patients second, when prescribing GLP-1s. This is because the demand is so high diabetics are having a hard time getting the medication. Side note: The dose for weight loss is higher than for diabetes.
🧃Will people stop eating convenience food and purchasing quick-fix programs and products? Before, people were vulnerable to the persuasion of a multi-billion-dollar weight-loss industry, the for-profit companies that have capitalized on weight loss – a supplement, a program, a pill.
Let’s not forget the lure of the convenience food industry and how it impacts this all. It’s hard to compete with quick and delicious, even if it’s unhealthy. Now GLP-1s might replace those weight loss programs and products. Will this be a case of cost shifting or will it result in spending more in general? Currently spending continues to increase on weight loss in general to close to 90 billion dollars.
🩺 Those who are taking GLP-1s will be monitored more closely by their doctors. This can be good in that doctors are more in tune with their patients and can help manage their co-morbidities and other issues. But, this will also be costly – doctor visits are expensive. I honestly don’t know how often someone needs to see their doctor once on the medication, so I need to find this out.
There is also a doctor shortage – what about the demand these medications place on doctors and what does this do to access to healthcare? Or will disease decline, thus helping doctors be able to see more patients? What about people who don’t have doctors who can prescribe GLP-1s nearby? I’m seeing this done via telemedicine – is this safe?
🪐 GLP-1 patients are individually working on weight loss in isolation (unless they’re part of some online support group). Chances are that they will revert to their old lifestyle habits if they don’t have social support. This has not yet been addressed that I know of.
🤤 Much of the weight is regained once medication is stopped, so this sets the stage for medication dependence. I have a lot of concerns about that.
As you can see, I had lots of questions. But they’re not the central focus of this exercise, and I had to re-shift my focus to the question at hand which is, “Would I take this medication or recommend it to others?”
Armed with my homework — the understanding of my own biases, emotions, and concerns — I realized my feelings were maybe stronger than I had realized on the topic. I’d have to temper these with facts and logical perspectives.
Okay, with that being out of the way, let’s keep going.
Here’s what I know, besides the fact that lifestyle modifications work most of the time for weight loss. Some clients are looking for a faster solution – a quick fix. These folks don’t want to work on lifestyle modifications– they excuse that option away for a variety of reasons, like they don’t like to cook, they’re too tired, they don’t have enough time, etc. (This is not conjecture– I have clients tell me this all the time.)
Many also feel that lifestyle modifications aren’t getting them results fast enough, and for some, not at all.
I also know that those who are overweight or obese have other health issues most of the time, and if this medication can control or negate some of these chronic issues, then that’s a win for sure. Perhaps some of these folks will get off of other medications. I wonder what the likelihood of that is (oops, another question).
What are the basics of GLP-1s that we should know?
What are GLP-1s for weight loss? Here you can find an explanation from a reliable source.
But to summarize, Glucagon Like Peptide-1 (shortened to GLP-1) is a term used to describe a class of medications that impact gut hormones - the hormones that are responsible for regulation secretion, absorption, motility, and digestion – all the things that guts do.

Image courtesy of GoodRX
There are a few of these on the market for diabetes and for weight loss and they have slightly different modes of action, of which some seem to be more effective. (If you’re looking to begin use of a GLP-1, talk to your doc and do your homework about which one is the right one for you and why.)
Ozempic is the diabetes drug, and Wegovy is technically the weight loss drug — it should be noted that both are semaglutides. These have also been referred to as STEP-1, as well as GLP-1’s.
Physiology fact: Did you know that the gut is the single largest endocrine organ in the body? These hormones in the gut hugely influence all our physiological systems to some degree (yes, including your nervous system – the gut has been called the “second brain” because it’s the most complex neural network outside the brain.)
Yet another question arose for me here… what do studies say about the impact of GLP-1s on mood and cognition, if anything? Do we know if GLP-1s will impact our mood?
My initial thought, is this: well, if we’re cutting fat and decreasing risk for cardiovascular disease and stroke, we are likely decreasing the chance of cognitive decline linked with obesity and risk factors for heart disease. Perhaps we’re also improving mood because we’re feeling better and we’re sleeping better? This needs more research, and I plan to return to it.

Photo courtesy of Knowable Magazine.
GLP-1s also influence the pancreas to produce insulin. That’s why they’re used for the management of diabetes.
A question I might want to look up or ask my doctor if I was seriously considering GLP-1s is, “Do all overweight / obese individuals struggle with insulin? Could some obese or overweight folks have normal insulin function? What does influencing the production of insulin do to someone with normal insulin function?”
Knowing that all hormones are related, I wasn’t surprised to hear that GLP-1 also impacted hormones in the brain, specifically ghrelin and leptin, the hormones that regulate hunger and fullness in the brain. This is why people aren’t as hungry and feel full after eating only a little.
Yet another question arose here: what else could these hormones be impacting that we should know about before we try GLP-1s? Also, should we consider our genetics as we look at trying it?
After doing some research, I found that people did lose significant amount of weight using GLP-1s – 14.9% for semaglutide and 15 – 20% with tirzepatide.
If I were wanting to lose weight, this would sound very appealing.
The recommendation for people to shift out of prediabetes is 7 - 10% weight loss (I was a certified National Diabetes Program Prevention lifestyle coach but let my certification expire over 10 years ago. I still offer DPP programs for my corporate clients and the guidelines haven’t changed. I have a vested interest in keeping people from getting diabetes, so in the aspect, GLP-1s hold promise.)
But interestingly, people regained weight, 6.9% for those on semaglutide, when stopping the GLP-1. So, one question I had was, “How long would someone have to stay on this medication?” The answers I found varied from ‘never’ to ‘it depends,’ but I can’t find information about set criteria for getting off the medication.
Note if you’re planning on trying this medication: Ask your doctor what the plan is for getting off GLP-1s, if there is one. This would impact my decision to take GLP-1s because I don’t want to rely on medication if I don’t have to, but that is my health philosophy. I would ask my client’s what they think about remaining on it indefinitely, should that be the recommendation.
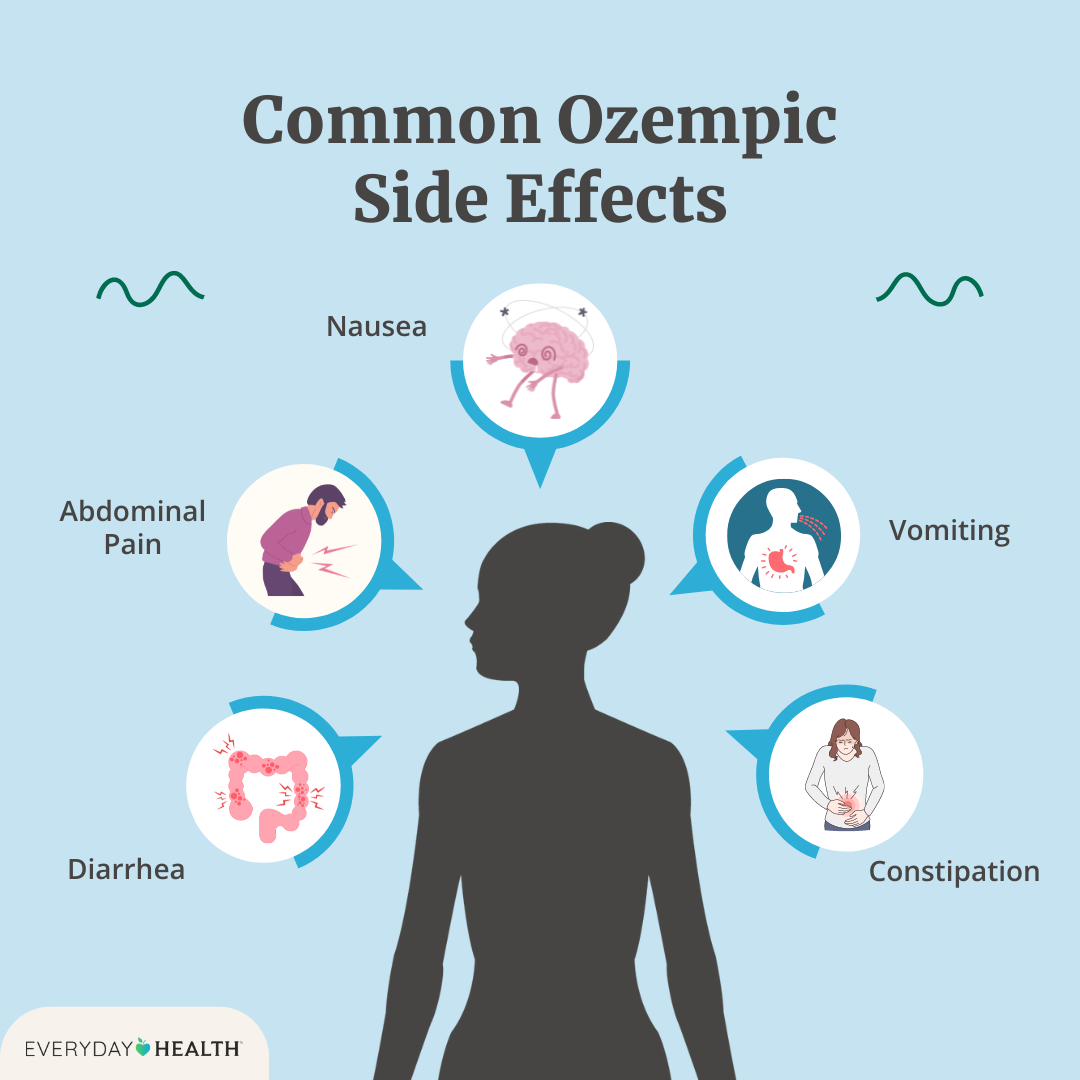
Photo courtesy of Everyday Health.
A look at some side effects.
Side effects are mild to moderate gastrointestinal side effects, including nausea, diarrhea, constipation, abdominal pain, and/or vomiting. There is also a concern of muscle mass decline when receiving GLP-1 treatment (25% to 40%), more than is lost when using traditional lifestyle interventions (15% - 20%).
When stopping GLP-1s, there is a risk of stronger feelings of hunger returning and thus leading to an increase in food consumption. I see one mention that compound forms of GLP-1s can result in unanticipated side effects. I spent about 10 minutes looking into this but did not find what exactly that means. I tried to find long-term effects of being GLP-1s and had a hard time finding anything concrete. Again, I shortened my research to 48 hours of that I only devoted maybe 6 hours at the most to learning more about GLP-1s.
Taking into account individual tolerances for Cost, Risk, Effectiveness, Effort, and Commitment (CREEC)
One of the tools I use for evaluating health decision options is CREEC, which stands for Cost, Risk, Efficacy, Effort, and Commitment.
When my clients find an option that they’re seriously considering, like GLP-1s, and they look at the facts and nuances to the point they feel they’ve done enough legwork (and is subjective and depends on each of our health decision making style – I created a way to find yours, just take this short 2 minute quiz), then I have them look at the option through the lens CREEC.
From my perspective, I’m seeing that:
(C) Cost is high.
(R) Risk is moderate. (In my opinion, short-term risk to health is low, side-effect risk is moderate, long-term risk is questionable)
(E) Effectiveness is high.
(E) Effort is low.
(C) Commitment is high (once you’re off of it, weight rebounds).
So, would I recommend my clients consider GLP-1s as an option for weight loss?
First, to be honest, I don’t make recommendations to my clients unless they ask. But if they asked, I would have to start by saying that I am bias and emotion heavy and I may not be able to provide objective input for my client to make an objective decision.
I would encourage them to also go through a 48-hour exercise of looking into the details that matter most to them. I would recommend they do this knowing their decision-making personality and CREEC tolerance levels to see where they stand on GLP-1s in light of those preferences.
Then I would ask some questions about why lifestyle management isn’t enough. If they decided to try GLP-1s, I would fully support their decision because they put in the work to look into making a well-considered health decision.
Would I take GLP-1s?
This is probably not a surprise, but no, I would not take GLP-1s — for many reasons.
The main one is that there isn’t enough known about this medication’s long-term impact, and it sets the patient up to be in the medical system for the long-term.
I’d rather not be in the medical system as much as possible, if I can help it, and I think I could in this case. I also have a health philosophy of not wanting to take medications unless I absolutely must. I’m very leery of side-effects of medications.
I would choose to double-down my efforts to try to manage my weight with lifestyle modifications. I would double down on my lifestyle modification efforts. I would find a personal trainer, health coach, dietician, or anyone else who could help me do so. It would be a cheaper than GLP-1s by far, but it would be more work on my part. I would be committed to do the work but would make sure I have the support I need, as well as accountability, and find ways to continue to keep my motivation.
If I had a lot of weight to lose, and if I had co-morbid conditions like heart disease or diabetes or sleep apnea, and my doctor showed concern and told me that if I didn’t do something soon, I might die prematurely, then I probably would consider it. But I would certainly add in the lifestyle management component because I would worry that access to the medication might be problematic, and I would want the weight loss to be sustainable.
I also would not want to be on the medication long-term, so I would hope that lifestyle management would prevent that from happening.

TL;DR
This represents a lot of work from a 48-hour dive into GLP-1s, but it honestly barely scratched the surface.
There are things missing – there’s a lot we don’t know about GLP-1s and their use in weight loss. This exercise isn’t perfect because there is no perfect way, but it was mostly logical in its approach to a large extent — much more so than most people partake in when considering a new approach to managing health.
I think this exercise can be used as a jumping-off point for others to ask their own questions and look further into the aspects that matter most to them.
My overall opinion is regarding GLP-1s is that…
👩🏽⚕️ Medical providers should be cautious to not be too quick to jump on the use of GLP-1s unless they are sure their clients have demonstrated that lifestyle management doesn’t produce the needed results to reduce or reverse associated chronic illness that comes with obesity.
🗒️ There should be classes or formal education for patients before they embark on GLP-1s, so they are fully aware of all aspects of this medication.
⏱️ Length of time on the medication needs to be clarified and justified.
💬 There needs to be more research and discussions around individual, societal, and social ramifications of this medication.
📊 Lack of data around long-term effects should be emphasized to patients embarking on GLP-1s.
🔦 I can’t imagine a typical patient going through this exercise before they decide to use GLP-1s, but they should! It’s unfair to offer such a medication without assisting patients to sort through the details and questions.
Whew! That was a marathon. If you’re interested in health decision making tools you can reach out to me directly. I’m always around in the comments and am super curious about your own experiences:
Are you on Ozempic, or have you ever been?
If so, how did/do you feel?
What are your thoughts?
Do you need help processing a difficult health issue? Are you ready to improve your health but don’t know where to begin? We offer health coaching, which is a great place to start. Check it out here.
On Instagram: @the.health.navigator
And learn more about Dr. Alice Burron at her website: draliceburron.com
Or via her personal Instagram: @dr_burron
You can even connect with her on LinkedIn, if you want to be professional about it. 👓
And if you’re not subscribed to our Substack, what are ya doing? It’s free, and packed full of useful tools to help you on your journey to better, faster healing.